Hypertension
– is an elevation of the blood pressure necessary to perfuse tissue
and organs. Elevated systemic blood pressure is usually defined as a
systolic reading greater than or equal to 140 mm Hg and a diastolic
reading greater than or equal to 90 mm Hg.
Etiology
A
specific cause of hypertension can be established in only 10-15% of
patients. It is important to consider specific causes in each case,
however, because some of them are amenable to definitive surgical
treatment: renal artery constriction, coarctation of the aorta,
pheochromocytoma, Cushing's disease, and primary aldosteronism.
Patient
in whom no specific cause of hypertension can be found are said to
have essential hypertension. In most cases, elevated blood pressure
is associated with an overall increase in resistance to flow of blood
through arterioles, while cardiac output is usually normal.
Meticulous investigation of autonomic nervous system function,
baroreceptor reflexes, the renin-angiotensin-aldosterone system, and
the kidney failed to identify a primary abnormality as the cause of
increased peripheral vascular resistance in the essential
hypertension. Elevated blood pressure is usually caused by a
combination of several abnormalities.
A
family history of hypertension increased the likelihood that an
individual will develop hypertensive disease. Essential hypertension
occurs four times more frequently among blacks than among whites, and
it occurs more often among middle-aged males than among middle-aged
females. Environmental factors such as stressful lifestyle, high
dietary intake of sodium, obesity, and smoking all further predispose
an individual to the occurrence of hypertension.
Physiology
of Hypertension
Arterial
blood pressure is regulated within a narrow range to provide adequate
perfusion of the tissues without causing damage to the vascular
system, particularly the arterial intima. Arterial blood pressure is
directly proportional to the product of the cardiac output and the
peripheral vascular resistance (BP = CO x PVR). In both normal and
hypertensive individuals, cardiac output and peripheral resistance
are controlled mainly by to overlapping control mechanisms: the
baroreflexes mediated by the sympathetic nervous system, and the
renin-angiotensin-aldosterone system. Most antihypertensive drugs
lower blood pressure by reducing cardiac output and/or decreasing
peripheral resistance.
A.
Baroreceptors and the sympathetic nervous system
Baroreflexes
involving the sympathetic nervous system are responsible for the
rapid moment-to-moment regulation of blood pressure. A fall in blood
pressure causes pressure-sensitive neurons (baroreceptors in the
aortic arch and carotid sinuses) to send fewer impulses to
cardiovascular centers in the spinal cord. This prompts a reflex
response of increased sympathetic and decreased parasympathetic
output to the heart and vasculature, resulting in vasoconstriction
and increased cardiac output. These changes result in a compensatory
rise in blood pressure.
B.
Renin-angiotensin-aldosterone system
The
kidney provides for the long-term control of blood pressure by
altering the blood volume. Baroreceptors in the kidney respond to
reduce arterial pressure (and to sympathetic stimulation of
β-adrenoceptors) by
releasing the enzyme renin. This predispose converts angiotensinogen
to angiotensin I, which is in turn converted to angiotensin II in the
presence of angiotensin converting enzyme (ACE). Angiotensing II is
the body's most potent circulating vasocontrictor, causing an
increase in blood pressure. Furthermore, angiotensin II stimulates
aldosterone secretion, leading to increased renal sodium reabsorption
and an increase in blood volume, which contribute to a further
increase in blood pressure.
Classification
of Hypertension Based on JNC 7
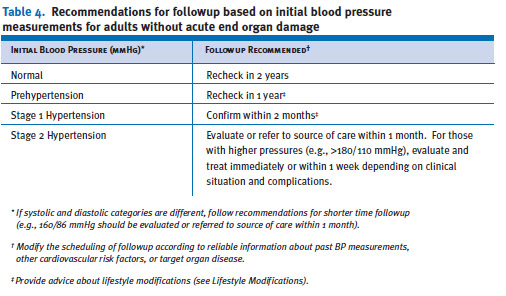
Table
4 provides a classification of BP for adults18 years and older. The
classification is based on the average of two or more properly
measured, seated, BP readings on each of two or more office visits.
Prehypertension
is not a
disease category. Rather, it is a designation chosen to identify
individuals at high
risk of developing hypertension, so that both patients and clinicians
are alerted to this risk and encouraged
to intervene and prevent or delay the disease from developing.
Individuals who are prehypertensive are not candidates for drug
therapy based on their level of BP and should be firmly and
unambiguously advised to practice lifestyle modification in order to
reduce their risk of developing hypertension in the future (see
Lifestyle Modifications). Moreover, individuals with prehypertension,
who also have
diabetes or kidney disease, should be considered candidates for
appropriate drug therapy if a trial of lifestyle modification fails
to reduce their BP to 130/80 mmHg or less.
This
classification does not stratify hypertensive individuals by the
presence or absence of risk factors
or target organ damage in order to make different treatment
recommendations, should either or
both be present. JNC 7 suggests that all
people with hypertension (stages 1 and
2) be treated. The treatment
goal for individuals with hypertension and no other compelling
conditions is <140/90 mmHg. The goal for individuals with
prehypertension and no compelling indications is to lower BP to
normal levels with lifestyle changes, and prevent the progressive
rise in BP using the recommended lifestyle modifications (see
Lifestyle Modifications).
Patient
Evaluation
 Evaluation
of hypertensive patients has three objectives: (1) to assess
lifestyle and identify other cardiovascular risk factors or
concomitant disorders that may affect prognosis and guide treatment
(table 6); (2) to reveal identifiable causes of high BP (table 7);
and (3) to assess the presence or absence of target organ damage and
CVD. Patient evaluation is made through medical history, physical
examination, routine laboratory tests, and other diagnostic
procedures. The physical examination should include: an appropriate
measurement of BP, with verification in the contralateral arm; an
examination of the optic fundi; a calculation of body mass index
(BMI) (measurement of waist circumference is also very useful); an
auscultation for carotid, abdominal, and femoral bruits; a palpation
of the thyroid gland; a thorough examination of the heart and lungs;
an examination of the abdomen for enlarged kidneys, masses, distended
urinary bladder, and abnormal aortic pulsation; a palpation of the
lower extremities for edema and pulses; and neurological assessment.
Evaluation
of hypertensive patients has three objectives: (1) to assess
lifestyle and identify other cardiovascular risk factors or
concomitant disorders that may affect prognosis and guide treatment
(table 6); (2) to reveal identifiable causes of high BP (table 7);
and (3) to assess the presence or absence of target organ damage and
CVD. Patient evaluation is made through medical history, physical
examination, routine laboratory tests, and other diagnostic
procedures. The physical examination should include: an appropriate
measurement of BP, with verification in the contralateral arm; an
examination of the optic fundi; a calculation of body mass index
(BMI) (measurement of waist circumference is also very useful); an
auscultation for carotid, abdominal, and femoral bruits; a palpation
of the thyroid gland; a thorough examination of the heart and lungs;
an examination of the abdomen for enlarged kidneys, masses, distended
urinary bladder, and abnormal aortic pulsation; a palpation of the
lower extremities for edema and pulses; and neurological assessment. Data
from epidemiological studies and clinical trials have demonstrated
that elevations in resting heart rate and reduced heart-rate
variability are associated with higher cardiovascular risk. In the
Framingham Heart Study, an average resting heart rate of 83 beats per
minute was associated with asubstantially higher risk of death from a
cardiovascular event than the risk associated with lower heart rate
levels. Moreover, reduced heart-rate variability was also associated
with an increase in cardiovascular mortality. No clinical trials have
prospectively evaluated the impact of reduced heart rate on
cardiovascular outcomes.
Data
from epidemiological studies and clinical trials have demonstrated
that elevations in resting heart rate and reduced heart-rate
variability are associated with higher cardiovascular risk. In the
Framingham Heart Study, an average resting heart rate of 83 beats per
minute was associated with asubstantially higher risk of death from a
cardiovascular event than the risk associated with lower heart rate
levels. Moreover, reduced heart-rate variability was also associated
with an increase in cardiovascular mortality. No clinical trials have
prospectively evaluated the impact of reduced heart rate on
cardiovascular outcomes.
Laboratory
Tests and Other Diagnostic Procedures
Routine
laboratory tests recommended before initiating therapy include a
12-lead electrocardiogram;
urinalysis;
blood glucose and hematocrit; serum potassium, creatinine (or the
corresponding estimated glomerular filtration rate [eGFR]), and
calcium;66 and a lipoprotein profile (after a 9- to 12-hour fast)
that includes high-density lipoprotein cholesterol (HDL-C),
low-density lipoprotein cholesterol (LDL-C), and triglycerides.
Optional tests include measurement of urinary albumin excretion or
albumin/creatinine ratio (ACR) except for those with diabetes or
kidney disease where annual measurements should be made. More
extensive testing for identifiable causes is not generally indicated
unless BP control is not achieved or the clinical and routine
laboratory evaluation strongly suggests an identifiable secondary
cause (i.e., vascular bruits, symptoms of catecholamine excess, or
unprovoked hypokalemia). (See Identifiable Causes of Hypertension for
a more thorough discussion.)
The
presence of decreased GFR or albuminuria has prognostic implications
as well. Studies reveal a strong relationship between decreases in
GFR and increases in cardiovascular morbidity and mortality. Even
small decreases in GFR increase cardiovascular risk. Serum creatinine
may overestimate glomerular filtration. The optimal tests to
determine GFR are debated, but calculating GFR from the recent
modifications of the Cockcroft and Gault
equations is useful. The presence of albuminuria, including
microalbuminuria, even in the setting of normal GFR, is also
associated with an increase in cardiovascular risk. Urinary albumin
excretion should be quantitated and monitored on an annual basis in
high-risk groups, such as those with diabetes or renal disease.
Additionally,
three emerging risk factors (1) high-sensitivity C-reactive protein
(HS-CRP); a marker of inflammation; (2) homocysteine; and (3)
elevated heart rate may be considered in some individuals,
particularly those with CVD but without other risk-factor
abnormalities. Results of an analysis of the Framingham Heart Study
cohort demonstrated that those with a LDL value within the range
associated with low cardiovascular risk, who also had an elevated
HS-CRP value, had a higher cardiovascular event rate as compared to
those with low CRP and high LDL cholesterol. Other studies also have
shown that elevated CRP is associated with a higher cardiovascular
event rate, especially in women. Elevations in homocysteine have also
been linked higher cardiovascular risk; however, the results with
this marker are not as robust as those with high
HS-CRP.
Identifiable
Causes of Hypertension
 Additional
diagnostic procedures may be indicated to identify causes of
hypertension, particularly in patients whose (1) age, history,
physical examination, severity of hypertension, or initial laboratory
findings suggest such causes; (2) BP responds poorly to drug therapy;
(3) BP begins to increase for uncertain reason after being well
controlled; and (4) onset of hypertension is sudden. Screening tests
for particular forms of identifiable hypertension are shown in table
8.
Additional
diagnostic procedures may be indicated to identify causes of
hypertension, particularly in patients whose (1) age, history,
physical examination, severity of hypertension, or initial laboratory
findings suggest such causes; (2) BP responds poorly to drug therapy;
(3) BP begins to increase for uncertain reason after being well
controlled; and (4) onset of hypertension is sudden. Screening tests
for particular forms of identifiable hypertension are shown in table
8.
Pheochromocytoma
should be suspected in patients with labile hypertension or with
paroxysms of hypertension accompanied by headache, palpitations,
pallor, and perspiration. Decreased pressure in the lower extremities
or delayed or absent femoral arterial pulses may indicate aortic
coarctation; and truncal obesity, glucose intolerance, and purple
striae suggest Cushing’s syndrome. Examples of clues from the
laboratory tests include unprovoked hypokalemia (primary
aldosteronism), hypercalcemia (hyperparathyroidism), and elevated
creatinine or abnormal urinalysis (renal
parenchymal disease). Appropriate investigations should be conducted
when there is a high index of suspicion of an identifiable cause.
The
most common parenchymal kidney diseases associated with hypertension
are chronic glomerulonephritis, polycystic kidney disease, and
hypertensive nephrosclerosis. These can generally be distinguished by
the clinical setting and additional testing. For example, a renal
ultrasound is useful
in
diagnosing polycystic kidney disease. Renal artery stenosis and
subsequent renovascular hypertension should be suspected in a number
of circumstances including: (1) onset of hypertension before age 30,
especially in the absence of family history, or onset of significant
hypertension
after
age 55; (2) an abdominal bruit especially if a diastolic component is
present; (3) accelerated hypertension; (4) hypertension that had been
easy to control but is now resistant; (5) recurrent flash
pulmonary
edema; (6) renal failure of uncertain etiology especially in the
absence of proteinuria or an abnormal urine sediment; and (7) acute
renal failure precipitated by therapy with an angiotensin converting
enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) under
conditions of occult bilateral renal artery stenosis or moderate to
severe volume depletion.
In
patients with suspected renovascular hypertension, noninvasive
screening tests include the ACEI-enhanced renal scan, duplex Doppler
flow studies, and magnetic resonance angiography. While renal artery
angiography remains the gold standard for identifying the anatomy of
the renal artery, it is not recommend for diagnosis alone because of
the risk associated with the procedure. At the time of intervention,
an arteriogram will be performed using limited contrast to confirm
the stenosis and identify the anatomy of the renal artery.
Goals
of Therapy
The
ultimate public health goal of antihypertensive therapy is to reduce
cardiovascular and renal morbidity and mortality. Since most persons
with hypertension, especially those >50 years of age, will reach
the DBP goal once the SBP goal is achieved, the primary focus should
be on attaining the SBP goal. Treating SBP and DBP to targets that
are <140/90 mmHg is associated with a decrease
in CVD complications. In patients with hypertension and
diabetes or renal disease, the BP goal is
<130/80 mmHg.
Therapeutic
Alternatives and Treatment
 There
are excellent clinical outcome trial data proving that lowering BP
with several classes of drugs, including angiotensin
converting enzyme inhibitors (ACEIs), angiotensin receptor blockers
(ARBs), beta-blockers (Bbs), calcium channel blockers (CCBs), and
thiazide-type diuretics, will all reduce the complications of
hypertension. Tables 10 and 11 provide a list of commonly used
antihypertensive agents.
There
are excellent clinical outcome trial data proving that lowering BP
with several classes of drugs, including angiotensin
converting enzyme inhibitors (ACEIs), angiotensin receptor blockers
(ARBs), beta-blockers (Bbs), calcium channel blockers (CCBs), and
thiazide-type diuretics, will all reduce the complications of
hypertension. Tables 10 and 11 provide a list of commonly used
antihypertensive agents. Thiazide-type
diuretics have been the basis of antihypertensive therapy in most
outcome trials. In these trials, including the recently published
Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack
Trial (ALLHAT),diuretics have been virtually unsurpassed in
preventing the cardiovascular complications of hypertension. The
exception is the Second Australian National Blood Pressure trial
which reported slightly better outcomes in White men with a regimen
that began with an ACEI compared to one starting with a diuretic.
Diuretics enhance the antihypertensive efficacy of multidrug
regimens, can be useful in achieving BP control, and are more
affordable than other antihypertensive agents. Despite these
findings, diuretics remain underutilized.
Thiazide-type
diuretics have been the basis of antihypertensive therapy in most
outcome trials. In these trials, including the recently published
Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack
Trial (ALLHAT),diuretics have been virtually unsurpassed in
preventing the cardiovascular complications of hypertension. The
exception is the Second Australian National Blood Pressure trial
which reported slightly better outcomes in White men with a regimen
that began with an ACEI compared to one starting with a diuretic.
Diuretics enhance the antihypertensive efficacy of multidrug
regimens, can be useful in achieving BP control, and are more
affordable than other antihypertensive agents. Despite these
findings, diuretics remain underutilized. Thiazide-type
diuretics should be used as initial therapy for most patients with
hypertension, either alone or in combination with one of the other
classes (ACEIs, ARBs, BBs, CCBs) demonstrated to be beneficial in
randomized controlled outcome trials. The list of compelling
indications requiring the use of other antihypertensive drugs as
initial therapy are listed in table 11. If a drug is not tolerated or
is contraindicated, then one of the other classes proven to reduce
cardiovascular events should be used instead.
Thiazide-type
diuretics should be used as initial therapy for most patients with
hypertension, either alone or in combination with one of the other
classes (ACEIs, ARBs, BBs, CCBs) demonstrated to be beneficial in
randomized controlled outcome trials. The list of compelling
indications requiring the use of other antihypertensive drugs as
initial therapy are listed in table 11. If a drug is not tolerated or
is contraindicated, then one of the other classes proven to reduce
cardiovascular events should be used instead.
Special
Considerations
The
patient with hypertension and certain comorbidities requires special
attention and followup by the clinician.
Ischemic
Heart Disease
Ischemic
heart disease (IHD) is the most common form of target organ damage
associated with hypertension. In patients with hypertension and
stable angina pectoris, the first drug of choice is usually a BB;
alternatively, long-acting CCBs can be used.In patients with acute
coronary syndromes (unstable angina or myocardial infarction),
hypertension should be treated initially with BBs and ACEIs, with
addition of other drugs as needed for BP control. In patients with
postmyocardial infarction, ACEIs, BBs, and aldosterone antagonists
have proven to be most beneficial. Intensive lipid management and
aspirin therapy are also indicated.
Heart
Failure
Heart
failure (HF), in the form of systolic or diastolic ventricular
dysfunction, results primarily from systolic hypertension and IHD.
Fastidious BP and cholesterol control are the primary preventive
measures for those at high risk for HF.In asymptomatic individuals
with demonstrable ventricular dysfunction, ACEIs and BBs are
recommended.For those with symptomatic ventricular dysfunction or
end-stage heart disease, ACEIs, BBs, ARBs and aldosterone blockers
are recommended along with loop diuretics.
Diabetic
Hypertension
Combinations
of two or more drugs are usually needed to achieve the target goal of
<130/80 mmHg.Thiazide diuretics, BBs, ACEIs, ARBs, and CCBs are
beneficial in reducing CVD and stroke incidence in patients with
diabetes. ACEI- or ARB-based treatments favorably affect the
progression of diabetic nephropathy and reduce albuminuria, and ARBs
have been shown to reduce progression to macroalbuminuria.
Chronic
Kidney Disease
In
people with chronic kidney disease (CKD), as defined by either (1)
reduced excretory function with an estimated GFR below 60 ml/min per
1.73 m2 (corresponding approximately to a creatinine of >1.5 mg/dL
in men or >1.3 mg/dL in women), or (2) the presence of
albuminuria (>300 mg/day or 200 mg albumin/g creatinine),
therapeutic goals are to slow deterioration of renal function and
prevent CVD. Hypertension appears in the majority of these patients,
and they should receive aggressive BP management, often with three or
more drugs to reach target BP values of <130/80 mmHg. ACEIs and
ARBs have demonstrated favorable effects on the progression of
diabetic and nondiabetic renal disease. A limited rise in serum
creatinine of as much as 35 percent above baseline with ACEIs or ARBs
is acceptable and is not a reason to withhold treatment unless
hyperkalemia develops. With advanced renal disease (estimated GFR <30
ml/min 1.73 m2, corresponding to a serum creatinine of 2.5–3
mg/dL), increasing doses of loop diuretics are usually needed in
combination with other drug classes.
Cerebrovascular
Disease
The
risks and benefits of acute lowering of BP during an acute stroke are
still unclear; control of BP at intermediate levels (approximately
160/100 mmHg) is appropriate until the condition has stabilized or
improved. Recurrent stroke rates are lowered by the combination of an
ACEI and thiazide-type diuretic.
Other
Special Situations
Minorities
BP
control rates vary in minority populations and are lowest in Mexican
Americans and Native Americans.1 In general, the treatment of
hypertension is similar for all demographic groups, but socioeconomic
factors and lifestyle may be important barriers to BP control in some
minority patients. The prevalence, severity, and impact of
hypertension are increased in African Americans, who also demonstrate
somewhat reduced BP responses to monotherapy with Bbs, ACEIs, or ARBs
compared to diuretics or CCBs. These differential responses are
largely eliminated by drug combinations that include adequate doses
of a diuretic. ACEI-induced angioedema occurs 2–4 times more
frequently in African American patients with hypertension than in
other groups.
Obesity
and the metabolic syndrome
Obesity
(BMI >30 kg/m2) is an increasingly prevalent risk factor for the
developmentof hypertension and CVD. The Adult Treatment Panel III
guideline for cholesterol management defines the metabolic syndrome
as the presence of three or more of the following conditions:
abdominal obesity (waist circumference >40 inches in men or >35
inches in women), glucose intolerance (fasting glucose >110
mg/dL), BP >130/85 mmHg, high triglycerides (>150 mg/dL), or
low HDL (<40 mg/dL in men or <50 mg/dL in women).66 Intensive
lifestyle modification should be pursued in all individuals with the
metabolic syndrome, and appropriate drug therapy should be instituted
for each of its components as indicated.
Left
ventricular hypertrophy
Left
ventricular hypertrophy (LVH) is an independent risk factor that
increases the risk of subsequent CVD. Regression of LVH occurs with
aggressive BP management, including weight loss, sodium restriction,
and treatment with all classes of antihypertensive agents except the
direct vasodilators hydralazine, and minoxidil.
Peripheral
arterial disease
Peripheral
arterial disease (PAD) is equivalent in risk to IHD. Any class of
antihypertensive drugs can be used in most PAD patients. Other risk
factors should be managed aggressively, and aspirin should be used.
Hypertension
in older persons
Hypertension
occurs in more than two-thirds of individuals after age 65. This is
also the population with the lowest rates of BP control. Treatment
recommendations for older people with hypertension, including those
who have isolated systolic hypertension, should follow the same
principles outlined for the general care of hypertension. In many
individuals, lower initial drug doses may be indicated to avoid
symptoms; however, standard doses and multiple drugs are needed in
the majority of older people to reach appropriate BP targets.
Postural
hypotension
A
decrease in standing SBP >10 mmHg, when associated with dizziness
or fainting,is more frequent in older patients with systolic
hypertension, diabetes, and those taking diuretics, venodilators
(e.g., nitrates, alpha-blockers, and sildenafillike drugs), and some
psychotropic drugs. BP in these individuals should also be monitored
in the upright position. Caution should be used to avoid volume
depletion and excessively rapid dose titration of antihypertensive
drugs.
Dementia
Dementia
and cognitive impairment occur more commonly in people with
hypertension. Reduced progression of cognitive impairment may occur
with effective antihypertensive therapy.
Hypertension
in women
Oral
contraceptives may increase BP, and the risk of hypertension
increases with duration of use. Women taking oral contraceptives
should have their BP checked regularly. Development of hypertension
is a reason to consider other forms of contraception. In contrast,
menopausal hormone therapy does not raise BP.
Women
with hypertension who become pregnant should be followed carefully
because of increased risks to mother and fetus. Methyldopa, BBs, and
vasodilators are preferred medications for the safety of the fetus.72
ACEI and ARBs should not be used during pregnancy because of the
potential for fetal defects and should be avoided in women who are
likely to become pregnant. Preeclampsia, which occurs after the 20th
week of pregnancy, is characterized by new-onset or worsening
hypertension, albuminuria, and hyperuricemia, sometimes with
coagulation abnormalities. In some patients, preeclampsia may develop
into a hypertensive urgency or emergency and may require
hospitalization, intensive monitoring, early fetal delivery, and
parenteral antihypertensive and anticonvulsant therapy.
Hypertension
in children and adolescents
In
children and adolescents, hypertension is defined as BP that is, on
repeated measurement, at the 95th percentile or greater adjusted for
age, height, and gender. The fifth Korotkoff sound is used to define
DBP. Clinicians should be alert to the possibility of identifiable
causes of hypertension in younger children (i.e., kidney disease,
coarctation of the aorta). Lifestyle interventions are strongly
recommended, with pharmacologic therapy instituted for higher levels
of BP or if there is insufficient response to lifestyle
modifications. Choices of antihypertensive drugs are similar in
children and adults, but effective doses for children are often
smaller and should be adjusted carefully. ACEIs and ARBs should not
be used in pregnant or sexually active girls. Uncomplicated
hypertension should not be a reason to restrict children from
participating in physical activities, particularly because long-term
exercise may lower BP. Use of anabolic steroids should be strongly
discouraged. Vigorous interventions also should be conducted for
other existing modifiable risk factors (e.g., smoking).
Hypertensive
urgencies and emergencies
Patients
with marked BP elevations and acute target-organ damage (e.g.,
encephalopathy, myocardial infarction, unstable angina, pulmonary
edema, eclampsia, stroke, head trauma, life-threatening arterial
bleeding, or aortic dissection)
require hospitalization and parenteral drug therapy.1 Patients with
markedly elevated BP but without acute target organ damage usually do
not require hospitalization, but they should receive immediate
combination oral antihypertensive therapy. They should be carefully
evaluated and monitored for hypertension-induced heart and kidney
damage and for identifiable causes of hypertension.
Additional
Considerations in Antihypertensive Drug Choices
Antihypertensive
drugs can have favorable or unfavorable effects on other
comorbidities.
Potential
favorable effects
Thiazide-type
diuretics are useful in slowing demineralization in osteoporosis. BBs
can be useful in the treatment of atrial
tachyarrhythmias/fibrillation, migraine, thyrotoxicosis (short term),
essential tremor, or perioperative hypertension. CCBs may be useful
in Raynaud’s syndrome and certain arrhythmias, and alpha-blockers
may be useful in prostatism.
Potential
unfavorable effects
Thiazide
diuretics should be used cautiously in patients who have gout or who
have a history of significant hyponatremia. BBs should generally be
avoided in individuals who have asthma, reactive airways disease, or
second or
third degree heart block. ACEIs and ARBs should not be given to women
likely to become pregnant and are contraindicated in those who are.
ACEIs should not be used in individuals with a history of angioedema.
Aldosterone antagonists and potassium-sparing diuretics can cause
hyperkalemia and should generally be avoided in patients who have
serum potassium values more than 5.0 mEq/L while not taking
medications.
Lifestyle
Modifications

Adoption
of healthy lifestyles by all persons is critical for the prevention
of high BP and is an indispensable part of the management of those
with hypertension. Weight loss of as little as
10 lbs (4.5 kg) reduces BP and/or prevents hypertension in a
large proportion of overweight persons, although the ideal is to
maintain normal body weight. BP is also benefited by adoption of the
Dietary Approaches to Stop Hypertension (DASH) eating plan which is a
diet rich in fruits, vegetables, and lowfat dairy products with a
reduced content of dietary cholesterol as well as saturated and total
fat (modification of whole diet). It is rich in potassium and calcium
content. Dietary sodium should be reduced to
no more than 100 mmol per day (2.4 g of sodium). Everyone who is able
should engage in regular aerobic physical activity such as brisk
walking at least 30 minutes per day most days of the week. Alcohol
intake should be limited to no more than 1 oz (30 mL) of ethanol, the
equivalent of two drinks per day in most men and no more than 0.5 oz
of ethanol (one drink) per day in women and lighter weight persons. A
drink is 12 oz of beer, 5 oz of wine, and 1.5 oz of 80- proof liquor
(see table 9). Lifestyle modifications reduce BP, prevent or delay
the incidence of hypertension, enhance antihypertensive drug
efficacy, and decrease cardiovascular risk. For example, in some
individuals, a 1,600 mg sodium DASH eating plan has BP effects
similar to single drug therapy. Combinations of two (or more)
lifestyle modifications can achieve even better results. For overall
cardiovascular risk reduction, patients should be strongly counseled
to quit smoking.
Followup
and Monitoring
Once
antihypertensive drug therapy is initiated, most patients should
return for followup and adjustment of medications at monthly
intervals or until the BP goal is reached. More frequent visits will
be necessary for patients with stage 2 hypertension or with
complicating comorbid conditions. Serum potassium and creatinine
should be monitored at least one to two times per year. After BP is
at goal and stable, followup visits can usually be at 3- to 6-month
intervals. Comorbidities such as HF, associated diseases such as
diabetes, and the need for laboratory tests influence the frequency
of visits. Other cardiovascular risk factors should be monitored and
treated to their respective goals, and tobacco avoidance must be
promoted vigorously. Low-dose aspirin therapy should be considered
only when BP is controlled because of the increased risk of
hemorrhagic stroke when the hypertension is not controlled.
Public
Health Challenges and Community Programs
Public
health approaches, such as reducing calories, saturated fat, and salt
in processed foods and increasing community/school opportunities for
physical activity, can achieve a downward shift in the distribution
of a population’s BP, thus potentially reducing morbidity,
mortality, and the lifetime risk of an individual’s becoming
hypertensive. This becomes especially critical as the increase in BMI
of Americans has reached epidemic levels. Now, 122 million adults are
overweight or obese, which contributes to the rise in BP and related
conditions. The JNC 7 endorses the American Public Health Association
resolution that the food manufacturers and restaurants reduce sodium
in the food supply by 50 percent over the next decade. When public
health intervention strategies address the diversity of racial,
ethnic, cultural, linguistic, religious, and social factors in the
delivery of their services, the likelihood of their acceptance by the
community increases. These public health approaches can provide an
attractive opportunity to interrupt and prevent the continuing costly
cycle of managing hypertension and its complications.
N.B. The
content is excerpt from The
Seventh Report of the Joint National Committee on
Prevention,
Detection, Evaluation, and Treatment of High Blood Pressure. For
complete information visit NHLBI
Web
site http://www.nhlbi.nih.gov/.