Sunday, June 30, 2013
US-FDA and Pharmacy Compounding
Note: Though in the Philippines community pharmacists do not much practice compounding anymore, it is essential to know that compounding medicines in other countries (like USA) is still valid and practiced. In the Philippines it is not totally eradicated as a function of community pharmacists, as a matter of fact some community pharmacies and hospital pharmacies are still compounding medicines but valid only when the treatment calls for a drug preparation that does not occur as pre-manufactured drug.
How to Dispose of Unused Medicines
Is your medicine cabinet filled with expired drugs or medications you no longer use? How should you dispose of them?
Most drugs can be thrown in the household trash, but consumers should take certain precautions before tossing them out, according to the Food and Drug Administration (FDA). A few drugs should be flushed down the toilet. And a growing number of community-based "take-back" programs offer another safe disposal alternative.
For example, the fentanyl patch, an adhesive patch that delivers a potent pain medicine through the skin, comes with instructions to flush used or leftover patches. Too much fentanyl can cause severe breathing problems and lead to death in babies, children, pets, and even adults, especially those who have not been prescribed the drug. "Even after a patch is used, a lot of the drug remains in the patch," says Hunter, "so you wouldn't want to throw something in the trash that contains a powerful and potentially dangerous narcotic that could harm others."
A company that wants FDA to approve its drug must submit
an application package to the agency. FDA requires, as part of the
application package, an assessment of how the drug's use would affect
the environment. Some drug applications are excluded from the assessment
requirement, says Bloom, based on previous agency actions.
"For those drugs for which environmental assessments have been required, there has been no indication of environmental effects due to flushing," says Bloom. In addition, according to the Environmental Protection Agency, scientists to date have found no evidence of adverse human health effects from pharmaceutical residues in the environment.
Nonetheless, FDA does not want to add drug residues into water systems unnecessarily, says Hunter. The agency reviewed its drug labels to identify products with disposal directions recommending flushing or disposal down the sink. This continuously revised listing can be found at FDA's Web page on Disposal of Unused Medicines.
Another environmental concern lies with inhalers used by people who have asthma or other breathing problems, such as chronic obstructive pulmonary disease. Traditionally, many inhalers have contained chlorofluorocarbons (CFC's), a propellant that damages the protective ozone layer. The CFC inhalers are being phased out and replaced with more environmentally friendly inhalers.
Depending on the type of product and where you live, inhalers and aerosol products may be thrown into household trash or recyclables, or may be considered hazardous waste and require special handling. Read the handling instructions on the label, as some inhalers should not be punctured or thrown into a fire or incinerator. To ensure safe disposal, contact your local trash and recycling facility.
Most drugs can be thrown in the household trash, but consumers should take certain precautions before tossing them out, according to the Food and Drug Administration (FDA). A few drugs should be flushed down the toilet. And a growing number of community-based "take-back" programs offer another safe disposal alternative.
Guidelines for Drug Disposal
FDA worked with the White House Office of National Drug Control Policy (ONDCP) to develop the first consumer guidance for proper disposal of prescription drugs. Issued by ONDCP in February 2007 and updated in October 2009, the federal guidelines are summarized here:- Follow any specific disposal instructions on the drug label or patient information that accompanies the medication. Do not flush prescription drugs down the toilet unless this information specifically instructs you to do so.
- Take advantage of community drug take-back programs that allow the public to bring unused drugs to a central location for proper disposal. Call your city or county government's household trash and recycling service (see blue pages in phone book) to see if a take-back program is available in your community. The Drug Enforcement Administration, working with state and local law enforcement agencies, is sponsoring National Prescription Drug Take Back Days throughout the United States.
- If
no instructions are given on the drug label and no take-back program is
available in your area, throw the drugs in the household trash, but
first:
- Take them out of their original containers and mix them with an undesirable substance, such as used coffee grounds or kitty litter. The medication will be less appealing to children and pets, and unrecognizable to people who may intentionally go through your trash.
- Put them in a sealable bag, empty can, or other container to prevent the medication from leaking or breaking out of a garbage bag.
- Before throwing out a medicine container, scratch out all identifying information on the prescription label to make it unreadable. This will help protect your identity and the privacy of your personal health information.
- Do not give medications to friends. Doctors prescribe drugs based on a person's specific symptoms and medical history. A drug that works for you could be dangerous for someone else.
- When in doubt about proper disposal, talk to your pharmacist.
Why the Precautions?
Disposal
instructions on the label are part of FDA's "risk mitigation" strategy,
says Capt. Jim Hunter, R.Ph., M.P.H., senior program manager on FDA's
Controlled Substance Staff. When a drug contains instructions to flush
it down the toilet, he says, it's because FDA, working with the
manufacturer, has determined this method to be the most appropriate
route of disposal that presents the least risk to safety.
Drugs
such as powerful narcotic pain relievers and other controlled substances
carry instructions for flushing to reduce the danger of unintentional
use or overdose and illegal abuse.For example, the fentanyl patch, an adhesive patch that delivers a potent pain medicine through the skin, comes with instructions to flush used or leftover patches. Too much fentanyl can cause severe breathing problems and lead to death in babies, children, pets, and even adults, especially those who have not been prescribed the drug. "Even after a patch is used, a lot of the drug remains in the patch," says Hunter, "so you wouldn't want to throw something in the trash that contains a powerful and potentially dangerous narcotic that could harm others."
Environmental Concerns
Despite
the safety reasons for flushing drugs, some people are questioning the
practice because of concerns about trace levels of drug residues found
in surface water, such as rivers and lakes, and in some community
drinking water supplies. However, the main way drug residues enter water
systems is by people taking medications and then naturally passing them
through their bodies, says Raanan Bloom, Ph.D., an environmental
assessment expert in FDA's Center for Drug Evaluation and Research.
"Most drugs are not completely absorbed or metabolized by the body, and
enter the environment after passing through waste water treatment
plants."
"For those drugs for which environmental assessments have been required, there has been no indication of environmental effects due to flushing," says Bloom. In addition, according to the Environmental Protection Agency, scientists to date have found no evidence of adverse human health effects from pharmaceutical residues in the environment.
Nonetheless, FDA does not want to add drug residues into water systems unnecessarily, says Hunter. The agency reviewed its drug labels to identify products with disposal directions recommending flushing or disposal down the sink. This continuously revised listing can be found at FDA's Web page on Disposal of Unused Medicines.
Another environmental concern lies with inhalers used by people who have asthma or other breathing problems, such as chronic obstructive pulmonary disease. Traditionally, many inhalers have contained chlorofluorocarbons (CFC's), a propellant that damages the protective ozone layer. The CFC inhalers are being phased out and replaced with more environmentally friendly inhalers.
Depending on the type of product and where you live, inhalers and aerosol products may be thrown into household trash or recyclables, or may be considered hazardous waste and require special handling. Read the handling instructions on the label, as some inhalers should not be punctured or thrown into a fire or incinerator. To ensure safe disposal, contact your local trash and recycling facility.
Pharmacy Compounding and the FDA: Questions and Answers
What is “compounding”?
Pharmacy compounding is a practice in which a licensed pharmacist combines, mixes, or alters ingredients of a drug in response to a prescription to create a medication tailored to the medical needs of an individual patient.Is combining two or more drugs considered compounding?
Yes, if it is done by a pharmacist in response to a licensed practitioner’s prescription and produces a medication tailored to an individual patient’s special medical needs.Why do some patients need compounded drugs?
Pharmacy compounding can serve an important public health need if a patient cannot be treated with an FDA-approved medication. Some examples of the need for compounding include:- If a patient has an allergy and needs a medication to be made without a certain dye.
- If an elderly patient or a child can’t swallow a pill and needs a medicine in a liquid form that is not otherwise available.
Are compounded drugs approved by the FDA?
Compounded drugs are not FDA-approved. This means that FDA does not verify the quality, safety and effectiveness of compounded drugs. This also means that compounded drugs lack an FDA finding of manufacturing quality. Consumers and health professionals rely on the drug approval process to ensure that drugs are safe and effective.Who regulates and inspects compounding pharmacies?
Each compounding pharmacy is licensed by its state’s board of pharmacy, which has primary responsibility for day-to-day oversight. The FDA's regulatory authority over certain compounding pharmacies is more limited than its authority over other drug manufacturers. For example, compounded drugs are not FDA approved. In addition, compounding pharmacies are not generally required to register with FDA and therefore do not tell FDA what drugs they are making.What are the risks associated with compounded drugs?
Compounded drugs can pose both direct and indirect health risks.- Direct health risks include unsafe compounded products. Compounded drugs made using poor quality compounding practices may be sub- or super‑potent, contaminated, or otherwise adulterated.
- Indirect health risks include the possibility that patients will use ineffective compounded drugs instead of FDA-approved drugs that have been shown to be safe and effective.
Does FDA want to prevent traditional pharmacy compounding?
No. FDA believes that pharmacists engaging in traditional pharmacy compounding provide a valuable medical service that is important to patient health.Note: Though in the Philippines community pharmacists do not much practice compounding anymore, it is essential to know that compounding medicines in other countries (like USA) is still valid and practiced. In the Philippines it is not totally eradicated as a function of community pharmacists, as a matter of fact some community pharmacies and hospital pharmacies are still compounding medicines but valid only when the treatment calls for a drug preparation that does not occur as pre-manufactured drug.
Don’t Double Up on Acetaminophen (Paracetamol)
You have flu symptoms, so you've been getting some relief for the
past two days by taking a cough and flu medicine every few hours. Late
in the day, you have a headache and you think about grabbing a couple of
acetaminophen tablets to treat the pain.
Stop right there.
What you may not realize is that more than 600 medications, both prescription and over-the-counter (OTC), contain the active ingredient acetaminophen to help relieve pain and reduce fever. Taken carefully and correctly, these medicines can be safe and effective. But taking too much acetaminophen can lead to severe liver damage.
Acetaminophen is a common medication for relieving mild to moderate pain from headaches, muscle aches, menstrual periods, colds and sore throats, toothaches, backaches and to reduce fever. It is also used in combination medicines, which have more than one active ingredient to treat more than one symptom.
Fathia Gibril, M.D., M.HSc., a supervisory medical officer at the Food and Drug Administration (FDA), explains that consumers looking for relief from a cold or the flu may not know that acetaminophen comes in combination with many other medications used to treat those symptoms. "So if you're taking more than one medicine at a time," she says, "you may be putting yourself at risk for liver damage."
Symptoms of acetaminophen overdose may take many days to appear, and even when they become apparent, they may mimic flu or cold symptoms. The current maximum recommended adult dose of acetaminophen is 4,000 milligrams per day, To avoid exceeding that dose:
FDA has an online list of brand names of products containing acetaminophen.
Even if you still have fever or pain, it's important not to take more than directed on the prescription or package label, notes FDA supervisory medical officer Sharon Hertz, M.D. But be careful, the word "acetaminophen" is not always spelled out in full on the container's prescription label. Abbreviations such as APAP, Acetaminoph, Acetaminop, Acetamin, or Acetam may be used instead.
When buying OTC products, Hertz suggests you make it a habit of telling the pharmacist what other medications and supplements you’re taking and asking if taking acetaminophen in addition is safe.
When the medicine is intended for children, the "Directions" section of the Drug Facts label tells you if the medicine is right for your child and how much to give. If a dose for your child's weight or age is not listed on the label and you can't tell how much to give, ask your pharmacist or doctor what to do.
If you're planning to use a medication containing acetaminophen, you should tell your health care professional if you have or have ever have had liver disease.
Acetaminophen and alcohol may not be a good mix, either, Hertz says. If you drink three or more alcoholic drinks a day, be sure to talk to your health care professional before you use a medicine containing acetaminophen. (USFDA)
Stop right there.
What you may not realize is that more than 600 medications, both prescription and over-the-counter (OTC), contain the active ingredient acetaminophen to help relieve pain and reduce fever. Taken carefully and correctly, these medicines can be safe and effective. But taking too much acetaminophen can lead to severe liver damage.
Acetaminophen is a common medication for relieving mild to moderate pain from headaches, muscle aches, menstrual periods, colds and sore throats, toothaches, backaches and to reduce fever. It is also used in combination medicines, which have more than one active ingredient to treat more than one symptom.
'Tis Cold and Flu Season
The National Institutes of Health (NIH) says that Americans catch one billion colds per year and as many as 20% of Americans get the flu. Moreover, 7 in 10 Americans use OTC medicines to treat cold, cough and flu symptoms.Fathia Gibril, M.D., M.HSc., a supervisory medical officer at the Food and Drug Administration (FDA), explains that consumers looking for relief from a cold or the flu may not know that acetaminophen comes in combination with many other medications used to treat those symptoms. "So if you're taking more than one medicine at a time," she says, "you may be putting yourself at risk for liver damage."
Symptoms of acetaminophen overdose may take many days to appear, and even when they become apparent, they may mimic flu or cold symptoms. The current maximum recommended adult dose of acetaminophen is 4,000 milligrams per day, To avoid exceeding that dose:
- don't take more than one OTC product containing acetaminophen,
- don't take a prescription and an OTC product containing acetaminophen, and
- don't exceed the recommended dose on any product containing acetaminophen.
FDA has an online list of brand names of products containing acetaminophen.
Rely on Health Care Experts
Acetaminophen is used in many commonly prescribed medications in combination with pain relievers such as codeine, oxycodone and hydrocodone. As of January 2011, FDA reported that overdoses from prescription medicines containing acetaminophen accounted for nearly half of all cases of acetaminophen-related liver injury in the U.S. When your health care professionals prescribe a drug, be sure to ask if it contains this active ingredient, and also to inform them of all other medicines (prescription and OTC) and supplements you take.Even if you still have fever or pain, it's important not to take more than directed on the prescription or package label, notes FDA supervisory medical officer Sharon Hertz, M.D. But be careful, the word "acetaminophen" is not always spelled out in full on the container's prescription label. Abbreviations such as APAP, Acetaminoph, Acetaminop, Acetamin, or Acetam may be used instead.
When buying OTC products, Hertz suggests you make it a habit of telling the pharmacist what other medications and supplements you’re taking and asking if taking acetaminophen in addition is safe.
When the medicine is intended for children, the "Directions" section of the Drug Facts label tells you if the medicine is right for your child and how much to give. If a dose for your child's weight or age is not listed on the label and you can't tell how much to give, ask your pharmacist or doctor what to do.
If you're planning to use a medication containing acetaminophen, you should tell your health care professional if you have or have ever have had liver disease.
Acetaminophen and alcohol may not be a good mix, either, Hertz says. If you drink three or more alcoholic drinks a day, be sure to talk to your health care professional before you use a medicine containing acetaminophen. (USFDA)
Ten Tips to Prevent an Accidental Overdose
For a medicine to work for you—and not against you—you’ve got to take the right dose.
Many over-the-counter liquid medicines—such as pain relievers, cold medicine, cough syrups, and digestion aids—come with spoons, cups, oral droppers, or syringes designed to help consumers measure the proper dose. These “dosage delivery devices” usually have measurement markings on them—such as teaspoons (tsp), tablespoons (tbsp), or milliliters (mL).
But the markings aren’t always clear or consistent with the directions on the medicine’s package. The Food and Drug Administration (FDA) has received numerous reports of accidental overdoses—especially in young children—that were attributed, in part, to the use of dosage delivery devices that were unclear or incompatible with the medicine’s labeled directions for use.
On May 4, 2011, FDA issued a guidance to firms that manufacture, market, or distribute over-the-counter liquid medicines. The guidance calls for them to provide dosage delivery devices with markings that are easy to use and understand.
Parents and caregivers can do their part, too, to avoid giving too much or too little of an over-the-counter medicine. Here are 10 tips:
Many over-the-counter liquid medicines—such as pain relievers, cold medicine, cough syrups, and digestion aids—come with spoons, cups, oral droppers, or syringes designed to help consumers measure the proper dose. These “dosage delivery devices” usually have measurement markings on them—such as teaspoons (tsp), tablespoons (tbsp), or milliliters (mL).
But the markings aren’t always clear or consistent with the directions on the medicine’s package. The Food and Drug Administration (FDA) has received numerous reports of accidental overdoses—especially in young children—that were attributed, in part, to the use of dosage delivery devices that were unclear or incompatible with the medicine’s labeled directions for use.
On May 4, 2011, FDA issued a guidance to firms that manufacture, market, or distribute over-the-counter liquid medicines. The guidance calls for them to provide dosage delivery devices with markings that are easy to use and understand.
Parents and caregivers can do their part, too, to avoid giving too much or too little of an over-the-counter medicine. Here are 10 tips:
- Always follow the directions on the Drug Facts label of your medicine. Read the label every time before you give the medicine.
- Know the "active ingredient" in the medicine. This is what makes the medicine work and it is always listed at the top of the Drug Facts label. Many medicines used to treat different symptoms have the same active ingredient. So if you're treating a cold and a headache with two different medicines but both have the same active ingredient, you could be giving two times the normal dose. If you're confused, check with a doctor, nurse, or pharmacist.
- Give the right medicine, in the right amount. Medicines with the same brand name can be sold in different strengths, such as infant, children, and adult formulas. The dose and directions also vary for children of different ages or weights. Always use the right strength and follow the directions exactly. Never use more medicine than directed unless your doctor tells you to do so.
- Talk to your doctor, pharmacist, or nurse to find out what mixes well and what doesn't. Medicines, vitamins, supplements, foods, and beverages aren’t always compatible.
- Use the dosage delivery device that comes with the medicine, such as a dropper or a dosing cup. A different device, or a kitchen spoon, could hold the wrong amount of medicine. And never drink liquid medicine from the bottle.
- Know the difference between a tablespoon (tbsp) and a teaspoon (tsp). A tablespoon holds three times as much medicine as a teaspoon. On measuring tools, a teaspoon (tsp) is equal to "5 mL."
- Know your child's weight. Dosage amounts for some medicines are based on weight. Never guess how much to give your child or try to figure it out from the adult dose instructions. If a dose is not listed for your child's weight, call your health care professional.
- Prevent a poison emergency by always using a child-resistant cap. Relock the cap after each use. Be especially careful with any medicines that contain iron; they are the leading cause of poisoning deaths in young children.
- Store all medicines in a safe place. Some are tasty, colorful, and many can be chewed. Kids may think they’re candy. Store all medicines and vitamins out of your child's (and your pet's) sight and reach. If your child takes too much, call the Poison Center Hotline at 800-222-1222 (open 24 hours a day, 7 days a week) or call 9-1-1.
- Check the medicine three times before using. For any medicine, it is always good practice to first, check the outside packaging for such things as cuts, slices, or tears. Second, once you’re at home, check the label on the inside package to be sure you have the right medicine and that the lid and seal are not broken. Third, check the color, shape, size, and smell. If you notice anything unusual, talk to a pharmacist or other health care professional before using.
Know Active Ingredients in Children's Meds
Ah-choo!
If your child is sneezing up a storm, it must be allergy season once more.
And if your child is taking more than one medication at the same time, there could be dangerous health consequences if those medicines have the same active ingredient, according to Hari Cheryl Sachs, M.D., a pediatrician at the Food and Drug Administration (FDA).
A medicine is made of many components. Some are "inactive" and only help it to taste better or dissolve faster, while others are active. An active ingredient in a medicine is the component that makes it pharmaceutically active—it makes the medicine effective against the illness or condition it is treating.
Active ingredients are listed first on a medicine's Drug Facts label for over-the-counter (OTC) products. For prescription medicines, they are listed in a patient package insert or consumer information sheet provided by the pharmacist.
Many medicines have just one active ingredient. But combination medicines, such as those for allergy, cough, or fever and congestion, may have more than one.
Take antihistamines taken for allergies. "Too much antihistamine can cause sedation and—paradoxically—agitation. In rare cases, it can cause breathing problems, including decreased oxygen or increased carbon dioxide in the blood, Sachs says.
"We're just starting allergy season," says Sachs. "Many parents may be giving their children at least one product with an antihistamine in it." Over-the-counter (OTC) antihistamines (with brand name examples) include diphenhydramine (Benadryl), chlorpheniramine (Chlor-Trimeton), clemastine (Tavist), fexofenadine (Allegra), loratadine (Claritin, Alavert), and cetirizine (Zyrtec).
But parents may also be treating their children for a separate ailment, such as a cough or cold. What they need to realize is that more than one combination medicine may be one too many.
"It's important not to inadvertently give your child a double dose," Sachs says.
Furthermore, two different active ingredients may serve the same purpose, Sachs says. For example, both acetaminophen and ibuprofen help reduce pain and fever. So there's generally no need to give your child both medicines for the same symptoms.
"It's easy to forget which medicines you're giving your child," Sachs says. "And if you have more than one child, it can get even more complicated." She recommends making it a habit to write down the name of any medicine you give your child, whether it's OTC or prescription (download a daily medicine records template).
"It's really a good idea to carry that list with you when you go to see your pediatrician or even when you go to the pharmacy," she adds. You should also note whatever vitamins or supplements your child is taking, as these can interact unfavorably with certain medicines, too.
Most importantly, Sachs says parents should always read the Drug Facts label on OTC products, and the patient package insert or consumer information sheet that comes with prescription medicines, every time they're considering a medication for their child, even if they think they already know the ingredients. They should know that the ingredients can change without an obvious change in the packaging. And they should contact their health care professional with any questions.
This article appears on FDA's Consumer Updates page, which features the latest on all FDA-regulated products. (Excerpt from USFDA, March 12, 2013)
If your child is sneezing up a storm, it must be allergy season once more.
And if your child is taking more than one medication at the same time, there could be dangerous health consequences if those medicines have the same active ingredient, according to Hari Cheryl Sachs, M.D., a pediatrician at the Food and Drug Administration (FDA).
A medicine is made of many components. Some are "inactive" and only help it to taste better or dissolve faster, while others are active. An active ingredient in a medicine is the component that makes it pharmaceutically active—it makes the medicine effective against the illness or condition it is treating.
Active ingredients are listed first on a medicine's Drug Facts label for over-the-counter (OTC) products. For prescription medicines, they are listed in a patient package insert or consumer information sheet provided by the pharmacist.
Many medicines have just one active ingredient. But combination medicines, such as those for allergy, cough, or fever and congestion, may have more than one.
Take antihistamines taken for allergies. "Too much antihistamine can cause sedation and—paradoxically—agitation. In rare cases, it can cause breathing problems, including decreased oxygen or increased carbon dioxide in the blood, Sachs says.
"We're just starting allergy season," says Sachs. "Many parents may be giving their children at least one product with an antihistamine in it." Over-the-counter (OTC) antihistamines (with brand name examples) include diphenhydramine (Benadryl), chlorpheniramine (Chlor-Trimeton), clemastine (Tavist), fexofenadine (Allegra), loratadine (Claritin, Alavert), and cetirizine (Zyrtec).
But parents may also be treating their children for a separate ailment, such as a cough or cold. What they need to realize is that more than one combination medicine may be one too many.
"It's important not to inadvertently give your child a double dose," Sachs says.
Other Health Complications
The same goes for other active ingredients, often found in combination products for allergies but also used to treat other symptoms, such as fever, headache or nasal congestion:- Acetaminophen (in Tylenol and many other products), a pain reliever often used to treat fevers, mild pain or headache. Taking too much can cause liver damage.
- Ibuprofen (for example, Advil or Motrin), another common medicine for relieving mild to moderate pain from headaches, sinus pressure, muscle aches and flu, as well as to reduce fever. Too much ibuprofen can cause nausea, vomiting, diarrhea, severe stomach pain, even kidney failure.
- Decongestants such as pseudoephedrine or phenylephrine (found in brand name drugs such as Actifed and Sudafed) taken in large amounts can cause excessive drowsiness in children. They can also cause heart rhythm disturbances, especially if combined with products and foods containing caffeine. In the form of nasal sprays and nose drops, these products, as well as oxymetazoline (the active ingredients in products such as Afrin), can cause "rebound" congestion, in which the nose remains stuffy or gets even worse.
Furthermore, two different active ingredients may serve the same purpose, Sachs says. For example, both acetaminophen and ibuprofen help reduce pain and fever. So there's generally no need to give your child both medicines for the same symptoms.
Write It All Down
Whether you're treating your child's condition with OTC medicines from the drug store or ones prescribed by your doctor, it's essential that you keep track of every medicine and the active ingredients each contains, Sachs says."It's easy to forget which medicines you're giving your child," Sachs says. "And if you have more than one child, it can get even more complicated." She recommends making it a habit to write down the name of any medicine you give your child, whether it's OTC or prescription (download a daily medicine records template).
"It's really a good idea to carry that list with you when you go to see your pediatrician or even when you go to the pharmacy," she adds. You should also note whatever vitamins or supplements your child is taking, as these can interact unfavorably with certain medicines, too.
Most importantly, Sachs says parents should always read the Drug Facts label on OTC products, and the patient package insert or consumer information sheet that comes with prescription medicines, every time they're considering a medication for their child, even if they think they already know the ingredients. They should know that the ingredients can change without an obvious change in the packaging. And they should contact their health care professional with any questions.
This article appears on FDA's Consumer Updates page, which features the latest on all FDA-regulated products. (Excerpt from USFDA, March 12, 2013)
Know the Risks of Indoor Tanning
Using ultraviolet (UV) tanning lamps, like those used in indoor
tanning beds, increases the risk of skin damage, skin cancer and eye
injury, according to the Food and Drug Administration (FDA) and numerous
other health organizations.
According to the American Cancer Society, melanoma—the deadliest form of skin cancer—accounted for 75,000 cases of skin cancer in 2012. According to the American Academy of Dermatology, indoor tanners are 75 percent more likely to develop melanoma than those who have never tanned indoors, and the risk increases with use.
To help protect consumers from the risks of indoor tanning, FDA is proposing changes in its regulation of sunlamps. The proposals are to enhance oversight of these devices, and to require labeling to include a recommendation designed to warn young people under the age of 18 not to use these devices.
This is due to concerns about long-term effects of exposure to dangerous UV rays. Because the effects add up over a lifetime, UV exposure in children and teenagers puts them at greater risk for skin and eye damage later in life.
Based on new risk information and recommendations from experts at an earlier FDA Medical Device Advisory Committee meeting, the agency is proposing to reclassify these devices from Class I to Class II. FDA can exert more regulatory control over Class II devices, notes FDA medical device expert Neil Ogden.
For example, sunlamps would have to undergo premarket review and comply with requirements relating to performance testing, software validation and biocompatibility. "We believe the reclassification will not only strengthen oversight of sunlamp products, but also will ensure that consumers are better informed about and protected from this sort of exposure," he explains.
In addition, FDA is proposing that manufacturers add a label to the sunlamp warning young people not to use these devices. The World Health Organization, the American Academy of Pediatrics, the American Academy of Dermatology, the American Medical Association and other organizations have previously supported what the FDA is now proposing: a recommendation that minors refrain from indoor tanning.
The proposed order will be published in the Federal Register at www.regulations.gov and FDA will take public comments for 90 days.
FDA also is proposing that sunlamp product labeling include a warning that people who are repeatedly exposed to sunlamp products see their health care professional on a regular basis to check for possible skin cancer.
The overview in Pediatrics suggests that doses of UV-A ultraviolet radiation emitted by high pressure tanning units may be up to 10 to 15 times higher than that of the midday sun, an intense exposure not found in nature. UV-A rays penetrate to the deeper layers of the skin and are often associated with allergic reactions, such as a rash. This is not to say that tanning outdoors is a safe activity. WHO has classified all UV radiation as carcinogenic (cancer causing).
According to the American Cancer Society, melanoma—the deadliest form of skin cancer—accounted for 75,000 cases of skin cancer in 2012. According to the American Academy of Dermatology, indoor tanners are 75 percent more likely to develop melanoma than those who have never tanned indoors, and the risk increases with use.
To help protect consumers from the risks of indoor tanning, FDA is proposing changes in its regulation of sunlamps. The proposals are to enhance oversight of these devices, and to require labeling to include a recommendation designed to warn young people under the age of 18 not to use these devices.
This is due to concerns about long-term effects of exposure to dangerous UV rays. Because the effects add up over a lifetime, UV exposure in children and teenagers puts them at greater risk for skin and eye damage later in life.
Proposed Changes
FDA regulates sunlamp products (including tanning beds and booths) both as medical devices and radiation-emitting products. Manufacturers of sunlamps must comply with FDA regulations regarding these devices.Based on new risk information and recommendations from experts at an earlier FDA Medical Device Advisory Committee meeting, the agency is proposing to reclassify these devices from Class I to Class II. FDA can exert more regulatory control over Class II devices, notes FDA medical device expert Neil Ogden.
For example, sunlamps would have to undergo premarket review and comply with requirements relating to performance testing, software validation and biocompatibility. "We believe the reclassification will not only strengthen oversight of sunlamp products, but also will ensure that consumers are better informed about and protected from this sort of exposure," he explains.
In addition, FDA is proposing that manufacturers add a label to the sunlamp warning young people not to use these devices. The World Health Organization, the American Academy of Pediatrics, the American Academy of Dermatology, the American Medical Association and other organizations have previously supported what the FDA is now proposing: a recommendation that minors refrain from indoor tanning.
The proposed order will be published in the Federal Register at www.regulations.gov and FDA will take public comments for 90 days.
FDA also is proposing that sunlamp product labeling include a warning that people who are repeatedly exposed to sunlamp products see their health care professional on a regular basis to check for possible skin cancer.
Skin Cancer Risk
"There is increasing evidence that tanning in childhood to early adult life increases the risk of skin cancer, including melanoma," says FDA dermatologist Markham Luke, M.D. In fact, according to an overview of studies recently published in the journal Pediatrics, melanoma is the second most common cancer in women in their 20s and the third most common cancer in men in their 20s in the U.S. Luke adds that many experts believe that at least one cause is the increased use of sunlamp products by U.S. teenagers and young adults.The overview in Pediatrics suggests that doses of UV-A ultraviolet radiation emitted by high pressure tanning units may be up to 10 to 15 times higher than that of the midday sun, an intense exposure not found in nature. UV-A rays penetrate to the deeper layers of the skin and are often associated with allergic reactions, such as a rash. This is not to say that tanning outdoors is a safe activity. WHO has classified all UV radiation as carcinogenic (cancer causing).
Practices to Avoid
FDA's proposal seeks to provide a reasonable assurance of safety and to make prospective users of sunlamps aware of the risks they face. Certain practices involving sunlamps are especially dangerous. These include:- failing to wear goggles—this can lead to short- and long-term eye injury.
- starting with long exposures (close to the maximum time for the particular sunlamp), which can lead to burning. Because sunburn takes 6 to 48 hours to develop, you may not realize your skin is burned until it's too late.
- failing to follow manufacturer-recommended exposure times on the label for your skin type (some skin types should not tan with UV radiation at all, for example those with skin that burns easily and doesn't readily tan).
- tanning while using certain medications or cosmetics that may make you more sensitive to UV rays. Talk to your doctor or pharmacist first.
FDA approves the first non-hormonal treatment for hot flashes associated with menopause
The U.S. Food and Drug Administration today approved Brisdelle
(paroxetine)to treat moderate to severe hot flashes (vasomotor symptoms)
associated with menopause. Brisdelle, which contains the selective
serotonin reuptake inhibitor paroxetine mesylate, is currently the only
non-hormonal treatment for hot flashes approved by the FDA.
There
are a variety of FDA-approved treatments for hot flashes, but all
contain either estrogen alone or estrogen plus a progestin.
Hot
flashes associated with menopause occur in up to 75 percent of women
and can persist for up to five years, or even longer in some women. Hot
flashes are not life-threatening, but the symptoms can be very
bothersome, causing discomfort, embarrassment and disruption of sleep.
“There
are a significant number of women who suffer from hot flashes
associated with menopause and who cannot or do not want to use hormonal
treatments,” said Hylton V. Joffe, M.D., M.M.Sc., director of the
Division of Bone, Reproductive and Urologic Products in the FDA’s Center
for Drug Evaluation and Research. “Today’s approval provides women with
the first FDA-approved, non-hormonal therapeutic option to help ease
the hot flashes that are so common in menopause.”
The
safety and effectiveness of Brisdelle were established in two
randomized, double-blind, placebo-controlled studies in a total of 1,175
postmenopausal women with moderate to severe hot flashes (a minimum of
seven to eight per day or 50-60 per week). The treatment period lasted
12 weeks in one study and 24 weeks in the other study. The results
showed that Brisdelle reduced hot flashes compared to placebo. The
mechanism by which Brisdelle reduces hot flashes is unknown.
The most common side effects in patients treated with Brisdelle were headache, fatigue, and nausea/vomiting.
Brisdelle
contains 7.5 mg of paroxetine and is dosed once daily at bedtime. Other
medications such as Paxil and Pexeva contain higher doses of paroxetine
and are approved for treating conditions such as major depressive
disorder, obsessive-compulsive disorder, panic disorder and generalized
anxiety disorder. All medications that are approved for treating
depression, including Paxil and Pexeva, have a Boxed Warning about an
increased risk of suicide in children and young adults. Because
Brisdelle contains the same active ingredient as Paxil and Pexeva, a
Boxed Warning about suicidality is included in the Brisdelle label.
Additional
labeled warnings include a possible reduction in the effectiveness of
tamoxifen if both medications are used together, an increased risk of
bleeding, and a risk of developing serotonin syndrome (signs and
symptoms can include confusion, rapid heart rate, and high blood
pressure). Brisdelle will be dispensed with a Medication Guide that
informs patients of the most important information about the medication.
The Medication Guide will be distributed to patients each time the
prescription is refilled.
Consumers and health
care professionals are encouraged to report adverse reactions from the
use of Brisdelle to the FDA MedWatch Adverse Event Reporting program at www.fda.gov/MedWatch or by calling 1-800-FDA-1088.
Brisdelle
and Pexeva are marketed by Noven Therapeutics, LLC., based in Miami,
Fla. Paxil is marketed by GlaxoSmithKline, based in Philadelphia, Pa.
For more information:
USP Monograph Modernization Program
The FDA recognizes that there is an ongoing need to update and
modernize the methods contained in the United States Pharmacopeia –
National Formulary (USP-NF). In this respect, the FDA, with
representation across the Agency, has established a Monograph
Modernization Working Group that interfaces with the USP Monograph
Modernization Program.
The direct participation of the
pharmaceutical industry, and other interested stakeholders, in USP’s
Monograph Modernization Program is encouraged to assist in providing
updated public standards vital to strengthen efforts for both FDA and
USP to protect the public health. Paramount to this effort is the
submission of updated analytical methodology pertinent to a compendial
article, as well as materials which could be used for independent
validation. FDA encourages all stakeholders to fully support this
effort.
Further information to become an active participant in this process is available on USP’s website at http://www.usp.org/usp-nf/development-process/monograph-modernization. Additionally, information, to include periodic status reports on this effort, is available at http://www.usp.org/usp-nf/key-issues/monograph-modernization. (From USFDA)
Friday, June 28, 2013
PUBLIC HEALTH WARNING AGAINST RECEIVING UNAPPROVED STEM CELL PREPARATIONS IN NON-HEALTH FACILITIES
FDA Advisory No. 2013-012
The FDA has been receiving complaints
from the public and health professionals that stem cell therapies are
conducted in non-health facilities, such as hotel rooms.
The public is warned against receiving
stem cell preparations and therapies without prior regulatory
applications and approval from the Food and Drug Administration,
Department of Health. The following stem cell preparations require FDA
approval: a) genetically altered human adult and umbilical cord stem
cells, b) adipose or fat cells derived human stem cell, c) human cells,
tissues, and cellular and tissue-based products that are subjected to
genetic manipulation, and d) live animal embryonic, fetal, or adult stem
cells in parenteral form for human administration. The public is
further warned that FDA-DOH does not allow the creation, importation,
promotion, marketing and use of human embryos, human embryonic stem
cells and their derivatives, aborted human fetal stem cells and their
derivatives for human treatment and research, as well as plant parts
labeled as stem cells.
Patients who might receive stem cell
preparations and therapy without prior FDA-DOH approval run the risks
of contracting infectious diseases and severe complications which may
lead to permanent disabilities, physical deformities, serious iatrogenic
harm, autoimmune diseases and worst death, and without the benefit of
health insurance coverage.
All patients are advised to consult only
with duly-licenses medical practitioners who practice stem cell therapy
in health facilities that are approved by the DOH. Moreover, patients
are highly encouraged to verify with the FDA, Philippines, before
undergoing the procedures using our
info@fda.gov.ph. This health
warning and advice extend to all tourists who visit the Philippines for
their leisure needs as well as medical needs.
FDA Philippines: Ensuring Access of Filipino People to Safe, Effective and Affordable Essential Medicines and the Pharmacy Law of the Philippines
The FDA is concerned over the statement made by the Philippine
Pharmacists Association (PPhA) and the Drugstores Association of the
Philippines (DAP) last 13 April 2013 that warned the public over
drugstores that employ "ghost pharmacists", referring to absentee
registered pharmacists employed by unscrupulous drugstore owners. The
statement made by PPhA EVP, Dr. Yolanda Robles, that around 70% of the
owners in the CAMANAVA area have no pharmacists is alarming. The FDA
would like to assure the public that the FDA shall continue to make sure
that safe and effective medicines are available to consumers in the
CAMANAVA area and the rest of the country. The FDA further informs the
public that it has initiated series of activities to address "ghost
pharmacies" and acute shortage of dedicated community pharmacists that
have severely affected the DOH delivery of public health goods and
services and health outcomes.
To see the full Advisory please click here: FDA Advisory No. 2013-011
Excerpt from FDA Philippines
Hypertension and Drug Therapy
Hypertension
– is an elevation of the blood pressure necessary to perfuse tissue
and organs. Elevated systemic blood pressure is usually defined as a
systolic reading greater than or equal to 140 mm Hg and a diastolic
reading greater than or equal to 90 mm Hg.
Etiology
A
specific cause of hypertension can be established in only 10-15% of
patients. It is important to consider specific causes in each case,
however, because some of them are amenable to definitive surgical
treatment: renal artery constriction, coarctation of the aorta,
pheochromocytoma, Cushing's disease, and primary aldosteronism.
Patient
in whom no specific cause of hypertension can be found are said to
have essential hypertension. In most cases, elevated blood pressure
is associated with an overall increase in resistance to flow of blood
through arterioles, while cardiac output is usually normal.
Meticulous investigation of autonomic nervous system function,
baroreceptor reflexes, the renin-angiotensin-aldosterone system, and
the kidney failed to identify a primary abnormality as the cause of
increased peripheral vascular resistance in the essential
hypertension. Elevated blood pressure is usually caused by a
combination of several abnormalities.
A
family history of hypertension increased the likelihood that an
individual will develop hypertensive disease. Essential hypertension
occurs four times more frequently among blacks than among whites, and
it occurs more often among middle-aged males than among middle-aged
females. Environmental factors such as stressful lifestyle, high
dietary intake of sodium, obesity, and smoking all further predispose
an individual to the occurrence of hypertension.
Physiology
of Hypertension
Arterial
blood pressure is regulated within a narrow range to provide adequate
perfusion of the tissues without causing damage to the vascular
system, particularly the arterial intima. Arterial blood pressure is
directly proportional to the product of the cardiac output and the
peripheral vascular resistance (BP = CO x PVR). In both normal and
hypertensive individuals, cardiac output and peripheral resistance
are controlled mainly by to overlapping control mechanisms: the
baroreflexes mediated by the sympathetic nervous system, and the
renin-angiotensin-aldosterone system. Most antihypertensive drugs
lower blood pressure by reducing cardiac output and/or decreasing
peripheral resistance.
A.
Baroreceptors and the sympathetic nervous system
Baroreflexes
involving the sympathetic nervous system are responsible for the
rapid moment-to-moment regulation of blood pressure. A fall in blood
pressure causes pressure-sensitive neurons (baroreceptors in the
aortic arch and carotid sinuses) to send fewer impulses to
cardiovascular centers in the spinal cord. This prompts a reflex
response of increased sympathetic and decreased parasympathetic
output to the heart and vasculature, resulting in vasoconstriction
and increased cardiac output. These changes result in a compensatory
rise in blood pressure.
B.
Renin-angiotensin-aldosterone system
The
kidney provides for the long-term control of blood pressure by
altering the blood volume. Baroreceptors in the kidney respond to
reduce arterial pressure (and to sympathetic stimulation of
β-adrenoceptors) by
releasing the enzyme renin. This predispose converts angiotensinogen
to angiotensin I, which is in turn converted to angiotensin II in the
presence of angiotensin converting enzyme (ACE). Angiotensing II is
the body's most potent circulating vasocontrictor, causing an
increase in blood pressure. Furthermore, angiotensin II stimulates
aldosterone secretion, leading to increased renal sodium reabsorption
and an increase in blood volume, which contribute to a further
increase in blood pressure.
Classification
of Hypertension Based on JNC 7
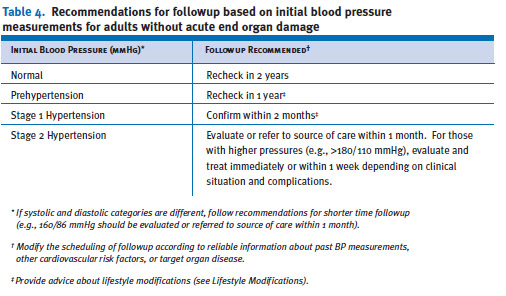
Table
4 provides a classification of BP for adults18 years and older. The
classification is based on the average of two or more properly
measured, seated, BP readings on each of two or more office visits.
Prehypertension
is not a
disease category. Rather, it is a designation chosen to identify
individuals at high
risk of developing hypertension, so that both patients and clinicians
are alerted to this risk and encouraged
to intervene and prevent or delay the disease from developing.
Individuals who are prehypertensive are not candidates for drug
therapy based on their level of BP and should be firmly and
unambiguously advised to practice lifestyle modification in order to
reduce their risk of developing hypertension in the future (see
Lifestyle Modifications). Moreover, individuals with prehypertension,
who also have
diabetes or kidney disease, should be considered candidates for
appropriate drug therapy if a trial of lifestyle modification fails
to reduce their BP to 130/80 mmHg or less.
This
classification does not stratify hypertensive individuals by the
presence or absence of risk factors
or target organ damage in order to make different treatment
recommendations, should either or
both be present. JNC 7 suggests that all
people with hypertension (stages 1 and
2) be treated. The treatment
goal for individuals with hypertension and no other compelling
conditions is <140/90 mmHg. The goal for individuals with
prehypertension and no compelling indications is to lower BP to
normal levels with lifestyle changes, and prevent the progressive
rise in BP using the recommended lifestyle modifications (see
Lifestyle Modifications).
Patient
Evaluation
 Evaluation
of hypertensive patients has three objectives: (1) to assess
lifestyle and identify other cardiovascular risk factors or
concomitant disorders that may affect prognosis and guide treatment
(table 6); (2) to reveal identifiable causes of high BP (table 7);
and (3) to assess the presence or absence of target organ damage and
CVD. Patient evaluation is made through medical history, physical
examination, routine laboratory tests, and other diagnostic
procedures. The physical examination should include: an appropriate
measurement of BP, with verification in the contralateral arm; an
examination of the optic fundi; a calculation of body mass index
(BMI) (measurement of waist circumference is also very useful); an
auscultation for carotid, abdominal, and femoral bruits; a palpation
of the thyroid gland; a thorough examination of the heart and lungs;
an examination of the abdomen for enlarged kidneys, masses, distended
urinary bladder, and abnormal aortic pulsation; a palpation of the
lower extremities for edema and pulses; and neurological assessment.
Evaluation
of hypertensive patients has three objectives: (1) to assess
lifestyle and identify other cardiovascular risk factors or
concomitant disorders that may affect prognosis and guide treatment
(table 6); (2) to reveal identifiable causes of high BP (table 7);
and (3) to assess the presence or absence of target organ damage and
CVD. Patient evaluation is made through medical history, physical
examination, routine laboratory tests, and other diagnostic
procedures. The physical examination should include: an appropriate
measurement of BP, with verification in the contralateral arm; an
examination of the optic fundi; a calculation of body mass index
(BMI) (measurement of waist circumference is also very useful); an
auscultation for carotid, abdominal, and femoral bruits; a palpation
of the thyroid gland; a thorough examination of the heart and lungs;
an examination of the abdomen for enlarged kidneys, masses, distended
urinary bladder, and abnormal aortic pulsation; a palpation of the
lower extremities for edema and pulses; and neurological assessment. Data
from epidemiological studies and clinical trials have demonstrated
that elevations in resting heart rate and reduced heart-rate
variability are associated with higher cardiovascular risk. In the
Framingham Heart Study, an average resting heart rate of 83 beats per
minute was associated with asubstantially higher risk of death from a
cardiovascular event than the risk associated with lower heart rate
levels. Moreover, reduced heart-rate variability was also associated
with an increase in cardiovascular mortality. No clinical trials have
prospectively evaluated the impact of reduced heart rate on
cardiovascular outcomes.
Data
from epidemiological studies and clinical trials have demonstrated
that elevations in resting heart rate and reduced heart-rate
variability are associated with higher cardiovascular risk. In the
Framingham Heart Study, an average resting heart rate of 83 beats per
minute was associated with asubstantially higher risk of death from a
cardiovascular event than the risk associated with lower heart rate
levels. Moreover, reduced heart-rate variability was also associated
with an increase in cardiovascular mortality. No clinical trials have
prospectively evaluated the impact of reduced heart rate on
cardiovascular outcomes.
Laboratory
Tests and Other Diagnostic Procedures
Routine
laboratory tests recommended before initiating therapy include a
12-lead electrocardiogram;
urinalysis;
blood glucose and hematocrit; serum potassium, creatinine (or the
corresponding estimated glomerular filtration rate [eGFR]), and
calcium;66 and a lipoprotein profile (after a 9- to 12-hour fast)
that includes high-density lipoprotein cholesterol (HDL-C),
low-density lipoprotein cholesterol (LDL-C), and triglycerides.
Optional tests include measurement of urinary albumin excretion or
albumin/creatinine ratio (ACR) except for those with diabetes or
kidney disease where annual measurements should be made. More
extensive testing for identifiable causes is not generally indicated
unless BP control is not achieved or the clinical and routine
laboratory evaluation strongly suggests an identifiable secondary
cause (i.e., vascular bruits, symptoms of catecholamine excess, or
unprovoked hypokalemia). (See Identifiable Causes of Hypertension for
a more thorough discussion.)
The
presence of decreased GFR or albuminuria has prognostic implications
as well. Studies reveal a strong relationship between decreases in
GFR and increases in cardiovascular morbidity and mortality. Even
small decreases in GFR increase cardiovascular risk. Serum creatinine
may overestimate glomerular filtration. The optimal tests to
determine GFR are debated, but calculating GFR from the recent
modifications of the Cockcroft and Gault
equations is useful. The presence of albuminuria, including
microalbuminuria, even in the setting of normal GFR, is also
associated with an increase in cardiovascular risk. Urinary albumin
excretion should be quantitated and monitored on an annual basis in
high-risk groups, such as those with diabetes or renal disease.
Additionally,
three emerging risk factors (1) high-sensitivity C-reactive protein
(HS-CRP); a marker of inflammation; (2) homocysteine; and (3)
elevated heart rate may be considered in some individuals,
particularly those with CVD but without other risk-factor
abnormalities. Results of an analysis of the Framingham Heart Study
cohort demonstrated that those with a LDL value within the range
associated with low cardiovascular risk, who also had an elevated
HS-CRP value, had a higher cardiovascular event rate as compared to
those with low CRP and high LDL cholesterol. Other studies also have
shown that elevated CRP is associated with a higher cardiovascular
event rate, especially in women. Elevations in homocysteine have also
been linked higher cardiovascular risk; however, the results with
this marker are not as robust as those with high
HS-CRP.
Identifiable
Causes of Hypertension
 Additional
diagnostic procedures may be indicated to identify causes of
hypertension, particularly in patients whose (1) age, history,
physical examination, severity of hypertension, or initial laboratory
findings suggest such causes; (2) BP responds poorly to drug therapy;
(3) BP begins to increase for uncertain reason after being well
controlled; and (4) onset of hypertension is sudden. Screening tests
for particular forms of identifiable hypertension are shown in table
8.
Additional
diagnostic procedures may be indicated to identify causes of
hypertension, particularly in patients whose (1) age, history,
physical examination, severity of hypertension, or initial laboratory
findings suggest such causes; (2) BP responds poorly to drug therapy;
(3) BP begins to increase for uncertain reason after being well
controlled; and (4) onset of hypertension is sudden. Screening tests
for particular forms of identifiable hypertension are shown in table
8.
Pheochromocytoma
should be suspected in patients with labile hypertension or with
paroxysms of hypertension accompanied by headache, palpitations,
pallor, and perspiration. Decreased pressure in the lower extremities
or delayed or absent femoral arterial pulses may indicate aortic
coarctation; and truncal obesity, glucose intolerance, and purple
striae suggest Cushing’s syndrome. Examples of clues from the
laboratory tests include unprovoked hypokalemia (primary
aldosteronism), hypercalcemia (hyperparathyroidism), and elevated
creatinine or abnormal urinalysis (renal
parenchymal disease). Appropriate investigations should be conducted
when there is a high index of suspicion of an identifiable cause.
The
most common parenchymal kidney diseases associated with hypertension
are chronic glomerulonephritis, polycystic kidney disease, and
hypertensive nephrosclerosis. These can generally be distinguished by
the clinical setting and additional testing. For example, a renal
ultrasound is useful
in
diagnosing polycystic kidney disease. Renal artery stenosis and
subsequent renovascular hypertension should be suspected in a number
of circumstances including: (1) onset of hypertension before age 30,
especially in the absence of family history, or onset of significant
hypertension
after
age 55; (2) an abdominal bruit especially if a diastolic component is
present; (3) accelerated hypertension; (4) hypertension that had been
easy to control but is now resistant; (5) recurrent flash
pulmonary
edema; (6) renal failure of uncertain etiology especially in the
absence of proteinuria or an abnormal urine sediment; and (7) acute
renal failure precipitated by therapy with an angiotensin converting
enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) under
conditions of occult bilateral renal artery stenosis or moderate to
severe volume depletion.
In
patients with suspected renovascular hypertension, noninvasive
screening tests include the ACEI-enhanced renal scan, duplex Doppler
flow studies, and magnetic resonance angiography. While renal artery
angiography remains the gold standard for identifying the anatomy of
the renal artery, it is not recommend for diagnosis alone because of
the risk associated with the procedure. At the time of intervention,
an arteriogram will be performed using limited contrast to confirm
the stenosis and identify the anatomy of the renal artery.
Goals
of Therapy
The
ultimate public health goal of antihypertensive therapy is to reduce
cardiovascular and renal morbidity and mortality. Since most persons
with hypertension, especially those >50 years of age, will reach
the DBP goal once the SBP goal is achieved, the primary focus should
be on attaining the SBP goal. Treating SBP and DBP to targets that
are <140/90 mmHg is associated with a decrease
in CVD complications. In patients with hypertension and
diabetes or renal disease, the BP goal is
<130/80 mmHg.
Therapeutic
Alternatives and Treatment
 There
are excellent clinical outcome trial data proving that lowering BP
with several classes of drugs, including angiotensin
converting enzyme inhibitors (ACEIs), angiotensin receptor blockers
(ARBs), beta-blockers (Bbs), calcium channel blockers (CCBs), and
thiazide-type diuretics, will all reduce the complications of
hypertension. Tables 10 and 11 provide a list of commonly used
antihypertensive agents.
There
are excellent clinical outcome trial data proving that lowering BP
with several classes of drugs, including angiotensin
converting enzyme inhibitors (ACEIs), angiotensin receptor blockers
(ARBs), beta-blockers (Bbs), calcium channel blockers (CCBs), and
thiazide-type diuretics, will all reduce the complications of
hypertension. Tables 10 and 11 provide a list of commonly used
antihypertensive agents. Thiazide-type
diuretics have been the basis of antihypertensive therapy in most
outcome trials. In these trials, including the recently published
Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack
Trial (ALLHAT),diuretics have been virtually unsurpassed in
preventing the cardiovascular complications of hypertension. The
exception is the Second Australian National Blood Pressure trial
which reported slightly better outcomes in White men with a regimen
that began with an ACEI compared to one starting with a diuretic.
Diuretics enhance the antihypertensive efficacy of multidrug
regimens, can be useful in achieving BP control, and are more
affordable than other antihypertensive agents. Despite these
findings, diuretics remain underutilized.
Thiazide-type
diuretics have been the basis of antihypertensive therapy in most
outcome trials. In these trials, including the recently published
Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack
Trial (ALLHAT),diuretics have been virtually unsurpassed in
preventing the cardiovascular complications of hypertension. The
exception is the Second Australian National Blood Pressure trial
which reported slightly better outcomes in White men with a regimen
that began with an ACEI compared to one starting with a diuretic.
Diuretics enhance the antihypertensive efficacy of multidrug
regimens, can be useful in achieving BP control, and are more
affordable than other antihypertensive agents. Despite these
findings, diuretics remain underutilized. Thiazide-type
diuretics should be used as initial therapy for most patients with
hypertension, either alone or in combination with one of the other
classes (ACEIs, ARBs, BBs, CCBs) demonstrated to be beneficial in
randomized controlled outcome trials. The list of compelling
indications requiring the use of other antihypertensive drugs as
initial therapy are listed in table 11. If a drug is not tolerated or
is contraindicated, then one of the other classes proven to reduce
cardiovascular events should be used instead.
Thiazide-type
diuretics should be used as initial therapy for most patients with
hypertension, either alone or in combination with one of the other
classes (ACEIs, ARBs, BBs, CCBs) demonstrated to be beneficial in
randomized controlled outcome trials. The list of compelling
indications requiring the use of other antihypertensive drugs as
initial therapy are listed in table 11. If a drug is not tolerated or
is contraindicated, then one of the other classes proven to reduce
cardiovascular events should be used instead.
Special
Considerations
The
patient with hypertension and certain comorbidities requires special
attention and followup by the clinician.
Ischemic
Heart Disease
Ischemic
heart disease (IHD) is the most common form of target organ damage
associated with hypertension. In patients with hypertension and
stable angina pectoris, the first drug of choice is usually a BB;
alternatively, long-acting CCBs can be used.In patients with acute
coronary syndromes (unstable angina or myocardial infarction),
hypertension should be treated initially with BBs and ACEIs, with
addition of other drugs as needed for BP control. In patients with
postmyocardial infarction, ACEIs, BBs, and aldosterone antagonists
have proven to be most beneficial. Intensive lipid management and
aspirin therapy are also indicated.
Heart
Failure
Heart
failure (HF), in the form of systolic or diastolic ventricular
dysfunction, results primarily from systolic hypertension and IHD.
Fastidious BP and cholesterol control are the primary preventive
measures for those at high risk for HF.In asymptomatic individuals
with demonstrable ventricular dysfunction, ACEIs and BBs are
recommended.For those with symptomatic ventricular dysfunction or
end-stage heart disease, ACEIs, BBs, ARBs and aldosterone blockers
are recommended along with loop diuretics.
Diabetic
Hypertension
Combinations
of two or more drugs are usually needed to achieve the target goal of
<130/80 mmHg.Thiazide diuretics, BBs, ACEIs, ARBs, and CCBs are
beneficial in reducing CVD and stroke incidence in patients with
diabetes. ACEI- or ARB-based treatments favorably affect the
progression of diabetic nephropathy and reduce albuminuria, and ARBs
have been shown to reduce progression to macroalbuminuria.
Chronic
Kidney Disease
In
people with chronic kidney disease (CKD), as defined by either (1)
reduced excretory function with an estimated GFR below 60 ml/min per
1.73 m2 (corresponding approximately to a creatinine of >1.5 mg/dL
in men or >1.3 mg/dL in women), or (2) the presence of
albuminuria (>300 mg/day or 200 mg albumin/g creatinine),
therapeutic goals are to slow deterioration of renal function and
prevent CVD. Hypertension appears in the majority of these patients,
and they should receive aggressive BP management, often with three or
more drugs to reach target BP values of <130/80 mmHg. ACEIs and
ARBs have demonstrated favorable effects on the progression of
diabetic and nondiabetic renal disease. A limited rise in serum
creatinine of as much as 35 percent above baseline with ACEIs or ARBs
is acceptable and is not a reason to withhold treatment unless
hyperkalemia develops. With advanced renal disease (estimated GFR <30
ml/min 1.73 m2, corresponding to a serum creatinine of 2.5–3
mg/dL), increasing doses of loop diuretics are usually needed in
combination with other drug classes.
Cerebrovascular
Disease
The
risks and benefits of acute lowering of BP during an acute stroke are
still unclear; control of BP at intermediate levels (approximately
160/100 mmHg) is appropriate until the condition has stabilized or
improved. Recurrent stroke rates are lowered by the combination of an
ACEI and thiazide-type diuretic.
Other
Special Situations
Minorities
BP
control rates vary in minority populations and are lowest in Mexican
Americans and Native Americans.1 In general, the treatment of
hypertension is similar for all demographic groups, but socioeconomic
factors and lifestyle may be important barriers to BP control in some
minority patients. The prevalence, severity, and impact of
hypertension are increased in African Americans, who also demonstrate
somewhat reduced BP responses to monotherapy with Bbs, ACEIs, or ARBs
compared to diuretics or CCBs. These differential responses are
largely eliminated by drug combinations that include adequate doses
of a diuretic. ACEI-induced angioedema occurs 2–4 times more
frequently in African American patients with hypertension than in
other groups.
Obesity
and the metabolic syndrome
Obesity
(BMI >30 kg/m2) is an increasingly prevalent risk factor for the
developmentof hypertension and CVD. The Adult Treatment Panel III
guideline for cholesterol management defines the metabolic syndrome
as the presence of three or more of the following conditions:
abdominal obesity (waist circumference >40 inches in men or >35
inches in women), glucose intolerance (fasting glucose >110
mg/dL), BP >130/85 mmHg, high triglycerides (>150 mg/dL), or
low HDL (<40 mg/dL in men or <50 mg/dL in women).66 Intensive
lifestyle modification should be pursued in all individuals with the
metabolic syndrome, and appropriate drug therapy should be instituted
for each of its components as indicated.
Left
ventricular hypertrophy
Left
ventricular hypertrophy (LVH) is an independent risk factor that
increases the risk of subsequent CVD. Regression of LVH occurs with
aggressive BP management, including weight loss, sodium restriction,
and treatment with all classes of antihypertensive agents except the
direct vasodilators hydralazine, and minoxidil.
Peripheral
arterial disease
Peripheral
arterial disease (PAD) is equivalent in risk to IHD. Any class of
antihypertensive drugs can be used in most PAD patients. Other risk
factors should be managed aggressively, and aspirin should be used.
Hypertension
in older persons
Hypertension
occurs in more than two-thirds of individuals after age 65. This is
also the population with the lowest rates of BP control. Treatment
recommendations for older people with hypertension, including those
who have isolated systolic hypertension, should follow the same
principles outlined for the general care of hypertension. In many
individuals, lower initial drug doses may be indicated to avoid
symptoms; however, standard doses and multiple drugs are needed in
the majority of older people to reach appropriate BP targets.
Postural
hypotension
A
decrease in standing SBP >10 mmHg, when associated with dizziness
or fainting,is more frequent in older patients with systolic
hypertension, diabetes, and those taking diuretics, venodilators
(e.g., nitrates, alpha-blockers, and sildenafillike drugs), and some
psychotropic drugs. BP in these individuals should also be monitored
in the upright position. Caution should be used to avoid volume
depletion and excessively rapid dose titration of antihypertensive
drugs.
Dementia
Dementia
and cognitive impairment occur more commonly in people with
hypertension. Reduced progression of cognitive impairment may occur
with effective antihypertensive therapy.
Hypertension
in women
Oral
contraceptives may increase BP, and the risk of hypertension
increases with duration of use. Women taking oral contraceptives
should have their BP checked regularly. Development of hypertension
is a reason to consider other forms of contraception. In contrast,
menopausal hormone therapy does not raise BP.
Women
with hypertension who become pregnant should be followed carefully
because of increased risks to mother and fetus. Methyldopa, BBs, and
vasodilators are preferred medications for the safety of the fetus.72
ACEI and ARBs should not be used during pregnancy because of the
potential for fetal defects and should be avoided in women who are
likely to become pregnant. Preeclampsia, which occurs after the 20th
week of pregnancy, is characterized by new-onset or worsening
hypertension, albuminuria, and hyperuricemia, sometimes with
coagulation abnormalities. In some patients, preeclampsia may develop
into a hypertensive urgency or emergency and may require
hospitalization, intensive monitoring, early fetal delivery, and
parenteral antihypertensive and anticonvulsant therapy.
Hypertension
in children and adolescents
In
children and adolescents, hypertension is defined as BP that is, on
repeated measurement, at the 95th percentile or greater adjusted for
age, height, and gender. The fifth Korotkoff sound is used to define
DBP. Clinicians should be alert to the possibility of identifiable
causes of hypertension in younger children (i.e., kidney disease,
coarctation of the aorta). Lifestyle interventions are strongly
recommended, with pharmacologic therapy instituted for higher levels
of BP or if there is insufficient response to lifestyle
modifications. Choices of antihypertensive drugs are similar in
children and adults, but effective doses for children are often
smaller and should be adjusted carefully. ACEIs and ARBs should not
be used in pregnant or sexually active girls. Uncomplicated
hypertension should not be a reason to restrict children from
participating in physical activities, particularly because long-term
exercise may lower BP. Use of anabolic steroids should be strongly
discouraged. Vigorous interventions also should be conducted for
other existing modifiable risk factors (e.g., smoking).
Hypertensive
urgencies and emergencies
Patients
with marked BP elevations and acute target-organ damage (e.g.,
encephalopathy, myocardial infarction, unstable angina, pulmonary
edema, eclampsia, stroke, head trauma, life-threatening arterial
bleeding, or aortic dissection)
require hospitalization and parenteral drug therapy.1 Patients with
markedly elevated BP but without acute target organ damage usually do
not require hospitalization, but they should receive immediate
combination oral antihypertensive therapy. They should be carefully
evaluated and monitored for hypertension-induced heart and kidney
damage and for identifiable causes of hypertension.
Additional
Considerations in Antihypertensive Drug Choices
Antihypertensive
drugs can have favorable or unfavorable effects on other
comorbidities.
Potential
favorable effects
Thiazide-type
diuretics are useful in slowing demineralization in osteoporosis. BBs
can be useful in the treatment of atrial
tachyarrhythmias/fibrillation, migraine, thyrotoxicosis (short term),
essential tremor, or perioperative hypertension. CCBs may be useful
in Raynaud’s syndrome and certain arrhythmias, and alpha-blockers
may be useful in prostatism.
Potential
unfavorable effects
Thiazide
diuretics should be used cautiously in patients who have gout or who
have a history of significant hyponatremia. BBs should generally be
avoided in individuals who have asthma, reactive airways disease, or
second or
third degree heart block. ACEIs and ARBs should not be given to women
likely to become pregnant and are contraindicated in those who are.
ACEIs should not be used in individuals with a history of angioedema.
Aldosterone antagonists and potassium-sparing diuretics can cause
hyperkalemia and should generally be avoided in patients who have
serum potassium values more than 5.0 mEq/L while not taking
medications.
Lifestyle
Modifications

Adoption
of healthy lifestyles by all persons is critical for the prevention
of high BP and is an indispensable part of the management of those
with hypertension. Weight loss of as little as
10 lbs (4.5 kg) reduces BP and/or prevents hypertension in a
large proportion of overweight persons, although the ideal is to
maintain normal body weight. BP is also benefited by adoption of the
Dietary Approaches to Stop Hypertension (DASH) eating plan which is a
diet rich in fruits, vegetables, and lowfat dairy products with a
reduced content of dietary cholesterol as well as saturated and total
fat (modification of whole diet). It is rich in potassium and calcium
content. Dietary sodium should be reduced to
no more than 100 mmol per day (2.4 g of sodium). Everyone who is able
should engage in regular aerobic physical activity such as brisk
walking at least 30 minutes per day most days of the week. Alcohol
intake should be limited to no more than 1 oz (30 mL) of ethanol, the
equivalent of two drinks per day in most men and no more than 0.5 oz
of ethanol (one drink) per day in women and lighter weight persons. A
drink is 12 oz of beer, 5 oz of wine, and 1.5 oz of 80- proof liquor
(see table 9). Lifestyle modifications reduce BP, prevent or delay
the incidence of hypertension, enhance antihypertensive drug
efficacy, and decrease cardiovascular risk. For example, in some
individuals, a 1,600 mg sodium DASH eating plan has BP effects
similar to single drug therapy. Combinations of two (or more)
lifestyle modifications can achieve even better results. For overall
cardiovascular risk reduction, patients should be strongly counseled
to quit smoking.
Followup
and Monitoring
Once
antihypertensive drug therapy is initiated, most patients should
return for followup and adjustment of medications at monthly
intervals or until the BP goal is reached. More frequent visits will
be necessary for patients with stage 2 hypertension or with
complicating comorbid conditions. Serum potassium and creatinine
should be monitored at least one to two times per year. After BP is
at goal and stable, followup visits can usually be at 3- to 6-month
intervals. Comorbidities such as HF, associated diseases such as
diabetes, and the need for laboratory tests influence the frequency
of visits. Other cardiovascular risk factors should be monitored and
treated to their respective goals, and tobacco avoidance must be
promoted vigorously. Low-dose aspirin therapy should be considered
only when BP is controlled because of the increased risk of
hemorrhagic stroke when the hypertension is not controlled.
Public
Health Challenges and Community Programs
Public
health approaches, such as reducing calories, saturated fat, and salt
in processed foods and increasing community/school opportunities for
physical activity, can achieve a downward shift in the distribution
of a population’s BP, thus potentially reducing morbidity,
mortality, and the lifetime risk of an individual’s becoming
hypertensive. This becomes especially critical as the increase in BMI
of Americans has reached epidemic levels. Now, 122 million adults are
overweight or obese, which contributes to the rise in BP and related
conditions. The JNC 7 endorses the American Public Health Association
resolution that the food manufacturers and restaurants reduce sodium
in the food supply by 50 percent over the next decade. When public
health intervention strategies address the diversity of racial,
ethnic, cultural, linguistic, religious, and social factors in the
delivery of their services, the likelihood of their acceptance by the
community increases. These public health approaches can provide an
attractive opportunity to interrupt and prevent the continuing costly
cycle of managing hypertension and its complications.
N.B. The
content is excerpt from The
Seventh Report of the Joint National Committee on
Prevention,
Detection, Evaluation, and Treatment of High Blood Pressure. For
complete information visit NHLBI
Web
site http://www.nhlbi.nih.gov/.
Subscribe to:
Posts (Atom)